story concept of the day: a “medical mystery of the week” serial set in a world with monsters and superpowers and mutants and aliens
It would be like. One part comedy, one part drama, two parts world-building. The hospital has an aquatic wing for mermaids and sea monsters. How do you treat someone who has telepathic influenza? We’ll figure it out, I guess!
Some storyline concepts:
—a woman from a telepathic race based on anglerfish shows up in the ER in a panic because her mate, who is tiny and permanently attached to her body, has stopped communicating through their telepathic link
—the air-breathing doctors have to take over the aquatic ward after a mysterious illness spreads through the water-breathing staff
—an ambulance brings in an unconscious alien from a species totally outside of medical literature, the staff scramble to save their life while flying blind
—the first outbreak of lycanthropy in 50 years occurs following protests against the vaccine, the hospital is quarantined while the on-staff pharmacists try to control the situation
If I write this, I’d want it to be like. Scrubs meets WTNV.
Character concept: a demon who works in the ER because their ability to “steal” souls means they can bring back patients who are medically dead but still repairable if you can just get them breathing again.
He has some insanely generic sounding name like Doctor Fred and has that “snake tongue, fangs, ram horns, red skin, yellow eyes, long tail, black bat wings” thing going on
He’s like 35 and the object of unrepentant longing from most of the interns and junior staff. He’s kind and patient and great with kids and has the cutest hiccupy laugh and is absolutely the guy you want overseeing your training because he never yells. Everyone wants to marry Doctor Fred.
It’s a running joke that he’s probably a literal Incubus but there’s no aura or magic at play, he’s just got a perfect personality.
I think I’m naming this story “doctors and demons” for now
Another character is just. Nessie. The Loch Ness monster is here. She works at the front desk for the aquatic ward and pokes her head out of the water to pass notes and files to the other doctors.
One of the aquatic doctors is Doctor Lagoon, who is the creature from the black lagoon. He’s very intimidating but can be immediately be calmed down by bringing up his human wife or their daughter. There’s a picture of him holding his wife bridal style on his desk.
The actual protagonist is a human woman who considers herself totally normal but actually has SOME sort of powerful telekinesis that she constantly explains away as coincidence.
There’s a character named Cadaver or Caddie who is a living corpse that constantly regenerates. She’s vital to the hospital for organ transplants but an absolute nightmare for the staff because she does things like host speed dating for zombies in the morgue and eat everyone lunch out of the staff room fridge.
Also I think the protagonist’s name is Jane Doe or Doctor Doe, as a joke on her being average but… not at all.
I think the trio of main characters are Doctor Fred (emergency), Doctor Doe (in-patient) and an alien surgeon named Doctor Hive, who is close to an insectoid Cthulhu. A running joke is her ability to keep track of her hundreds of children but not the names of any of their fathers or her coworkers except her very favorites.
HAHAHA HOLY SHIT WE WERE LOOKING AT PICTURES OF SURGERIES IN CLASS AND ALL THE GUYS WERE HOOTING AT THE SLICED BREAST ONES AND THEN THE TEACHER SWITCHED TO A PENIS PIC WHERE IT WAS CUT OPEN AND SOME 300LB JOCK DOUCHEBAG FAINTED RIGHT OUT OF HIS CHAIR BOYS ARE WEAK BOYS ARE FUCKING WEAK
you mean to tell me
that there was a god damn CUT OPEN BOOB
IN SURGERY
AND BOYS WERE STILL SEXUALISING IT
FUCKING MOTHERFUCKING FUCK DOES NO ONE SEE HOW FUCKED UP THIS IS
When I took human anatomy, all the boys were *thrilled* to hold the breast implants, but when the professor brought out the jar of preserved penises we had no male volunteers to handle them. THEN she brought out the penis that had been dissected to show the different canals (it split into three more-or-less even sized pieces) and I think 3 boys went straight down like a sack of potatoes. Several more followed when she started pulling it apart and holding it up for the whole class to see. It was like that scene in Dracula Dead and Loving it where Mel Brooks is trying to gross out the med interns. Like, literally. It was hilarious.
Bonus: my anatomy professor (who is a woman) informed me that she had not once, in her 20 years of teaching the class, had a female fainter. Women are hardcore.
getting food poisoning is a sick irony. sandwich, you were supposed to nourish my fragile meat body, not conspire with one section of it to kill the rest. you edible brutus, you fredo, you fucking intestinal quisling
this post shows true literary prowess but i wish i hadn’t read it while finishing my sandwich
We all know what erectile dysfunction is but literally no one is ever taught what vaginismus is and it can cause people to feel extremely lost, broken, and cause people to take their own lives.
Raise. Awareness.
For the uninformed, vaginismus is when the vagina painfully tightens and spasms when faced with pressure, usually from anything trying to insert into the vagina. It’s the reason I can’t wear tampons, and why many people can’t have vaginal sex without severe pain.
There’s not a lot of treatments, and there isn’t a single one that is for vaginismus exclusively – they’re all medications or treatments to treat symptoms, but not the causes. In fact, for a long time doctors waved off vaginismus as a purely psychological disorder in cis women.
Seriously, this is so unaddressed and uncared for in medical circles. Please spread awareness, even if all it’s for is to let those who have it but don’t have a name for it finally be able to understand what’s happening to their bodies.
I’ve never even heard of this??
TMI moment: after I got a horrible, really painful pelvic examination by a male doctor (who didn’t seem at all concerned with how I felt and just kind of unceremoniously followed the procedure of having a female nurse present while he did it when I said I wouldn’t be comfortable instead of taking any measures to try and make the procedure more comfortable for me), I asked the doctor if it was a concern that I couldn’t use tampons or penetrative devices including the examination device without significant pain, like if it was normal or if I needed to be aware of any medical concerns associated with the issue. And this motherfucker told me that maybe I should see a psychiatrist to fix problems in my sex life. As in, he knew nothing about my sex life but was immediately willing to assume and tell me that my vaginal discomfort was a symptom of me being crazy and uptight and needing therapy so I could have sex with men. The medical world is just rampant with sexism and an absolute disregard for the pain and the physical and psychological wellbeing of women. I felt so deeply hurt and violated by the exam he gave me I wanted to cry every time I thought about it for weeks after and he was so bad at what he was doing that I was in a lot of physical pain for hours after the procedure, which absolutely Should Not happen when you get a pelvic exam but he was literally just that mean and rough with my vagina while I was actually crying with pain and he showed zero regard for how badly he was hurting me. And guess what, a week later I got another pelvic exam (because he gave me a medication that didn’t work for me and didn’t list the side effects so I got really sick and then the initial issue got worse), this time from a female doctor, and when I told her she got an extra small device and was extra gentle and it didn’t hurt because she had like the most basic level of human empathy and took the measures that existed to not hurt a woman in her care. But like, that’s the thing, the medical world is run largely by men and medical practitioners aren’t necessarily taught to have empathy for the feelings or even the overall health of women in their care, and in research levels too misogyny is hiding under the surface of the attitudes of much of the medical world. So it’s no wonder that issues related to vaginal and uterine reproductive health are never common knowledge and women’s sexual health is mainly seen even in medical circles as revolving around their ability to engage in sexual interaction with cis men.
I keep forgetting what the differences are in the over the counter pain relievers, so I made a handy chart.
This Is Important.
I always had really really horrible growing pains as a kid. Like, I clearly remember being curled up on the floor crying because it felt like some evil person had stuck a fork in my calf and was twisting it around like spaghetti. Mom always had me take ibuprofen for it, and when that didn’t do anything, she just gave me more.
Now the stuff barely works on me, even when I take it for the things it actually fixes.
Please, please, double-check to make sure you’re taking the right medicines for your pain.
My mom always gave me tylonel for period cramps as a kid and it never did anything. It’s nice to know now that she was literally giving me the least effective option
And please PLEASE note that as the chart says, acetaminophen “can be taken with NSAIDs”, which means you can take Tylenol/acetaminophen AND one of the other listed pain-relievers.
My mom has been a doctor for 40+ years, and her standard advice for headaches is, take two regular-strength Advil, and then if that doesn’t work, ALSO take two regular-strength Tylenol.
To summarize, a vagina can now be constructed from peritoneal tissue, meaning that it will self-lubricate, doesn’t require prior electrolysis, will be stretchier than one made from skin tissue, and doesn’t have any external grafting sites to worry about.
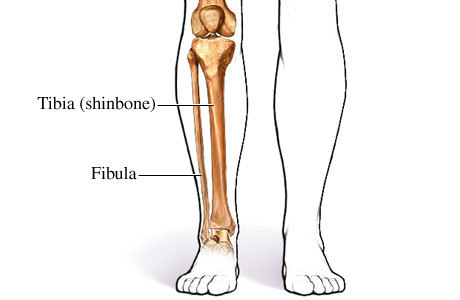
There are two bones in your lower leg. One’s big and buff and one’s pretty wimpy. When you walk, that big tibia takes ~80% of your weight of impact, and the fibula only has to take the remaining 20%.
But skaters place their weight differently over their feet. In principle a hockey player has 100% of their weight shifted forward onto their tibia.
You can actually see the implications of this in practice. If you break your fibula, 20% of the weight-bearing is gone, and you won’t really be able to walk. But a hockey player who cracks their fibula can and will keep skating almost without noticing something’s wrong. This happens pretty damn often when they block shots. You’ll see them skate easily over to get checked out, step up onto the hallway floor, and then suddenly slump over, with medical staff helping them limp off down the hallway.
I hear people saying, “oh, guess he’s fine!” when hockey players get up and appear to be skating okay: nah. And when a player wants to return to the ice: they may genuinely feel better skating but be too injured to walk.
And over time, if you’re in the weight-bearing position for skating more often than walking, and are skating from a young age, yes, that affects the shape of your weight-bearing bones and external appearance of your legs and feet. I don’t have a survey on hockey players’ shapely ankles compared to the normal population in front of me at the moment, but every single skater I see could be identified by their ankles
I thought this was going to be someone condescendingly explaining hockey to me but this is so informative and well written and I trust you with all my bones now.
Someone please source this, it’s too beautiful to not have sources
i can sort of provide some more explanation, maybe? note that all of my skating experience comes from taking figure skating lessons and that i am absolutely not a physiologist/sports science-person.
@brainsandbodies This wasn’t my original post, so I’m sorry I didn’t see you asking for sources earlier. All of you asking for sources here are very cool, and I wanted to round up what I can for you. If I forget somebody’s question, please just @ or ask me. But this also struck me because I think one of the most important things to remember about health is:
basic professional knowledge is often hard to cite and hard to make accessible
Hang with me for a sec.
This happens to be the story that got me into sports med. I’d just lost my parents; fuck knows what I was doing but I knew I needed to make up credit hours and I already had an EMT-B, so I signed up three weeks late for SM 136: Emergency Care, the first class I ever planned to sleep through. I remember coming in late for my first (late) day and seeing a lot of snapbacks in the room. It was taught by a small, sweet-faced man who used to train the Philadelphia Phillies: he’d fly down with the team to Tampa for spring training, so he got to know the head trainer for the Tampa Bay Lightning, and they got to gossiping about the shit their clients put them through.
When he got bored of baseball he left the Phillies, and moved up here to hockey country. He wanted to see some skaters break their legs.
He dragged us through the fundamentals of weight-bearing step by step, and you could see him light the fuck up: you just knew he was getting to something gross.
“So that’s how hockey players can break their own legs,” he said, stopping right by my desk, “and not even know it until they step off the ice. Fine, fine, and then—“ he made a wet sort of crunching noise. Whoever was under the snapback next to me gagged. I was hooked. I said, I believe, “COOL,” full-volume, and he met my eye, nodding with the full solemn grandeur of the wicked awesomeness of physiology.
You’re wondering: I got my first snapback that week.
Here’s the thing:
The fibula was found to bear about 6.4% of your weight when in a neutral ankle position in 1984. At the time the experiment had to be done with autopsy specimens and in simple positions (Takebe, Nakagawa, Minami, Kanazawa, Hirohata,1984). Since then we’ve seen that in the more complex positions of a standard heel-toe walking gait, the fibula typically carries about to 10-15% of a person’s weight and the tibia takes 80%. (It doesn’t add up because there are other tissues involved and the two bones work to stabilize each other.) 80% is the conventional approximation we’re taught in classes, that appears in biomedical textbooks, and that’s used in practice by therapists.
Most of the muscles of your calf and ankle attach to your fibula, so your fibula is all wrapped up snug in a bunch of muscle, so it follows that it’s hard to break. The conventional knowledge in healthcare is that people who come in with broken fibulas are athletes or were in motor vehicle accidents or were physically abused because that’s what we observe.
The risk of breaking your fibula is a casual part of how we talk about shot-blocking, because we see it happen a lot. And the Tampa Bay trainers who work directly with individual players had seen them skate off what turned out to be a broken fibula; my professor had seen it happen; I’ve seen it happen. It’s something that we talk about in classes and look for on the ice. But it’s kind of hard to study beyond the players you personally get your hands on.
Greg Campbell skated on what turned out to be a broken right fibula back in 2013.
But the only reason we have the footage of it was that it was an obvious, severe break, so he was in visible pain, and later the specific injury was made public. In other cases they don’t look especially hurt until they hit the hall, and the injury isn’t shared. So I can’t tell you how often it happens in total, out of all the hockey players out there. That information isn’t gathered anywhere.
Sports medicine is a fascinating and a bit of a fucked up field to try to explain because we have to use observational data and case studies and conventional knowledge.
We can’t line up a bunch of hockey players and whack them in the legs to see what happens in real time, or compare them to a control group who didn’t get whacked.* We can’t wait for people to be injured and round them all up to study, because it’s an unpredictable accident, and we can’t ask players to skate with an injury—that’s what I like to call “un-the-fuck-ethical.”
We’re also limited in how much we can see inside a living skater while they skate! Right now—like right now—motion-capture and 3D modeling is exploding our understanding of biomechanics, and that will inform PT practice. (There’s a reason Mathews and McDavid and all the other monsters are here now; we’re just now figuring out how to train them like that.)
But it’s still difficult even to gather data on how or how often certain injuries happen to certain people beyond individual trainers’ clinical observations. It’s not a centralized system. We don’t have concussion reporting worked out yet!
And it’s hard because it’s hard to get money to research something that’s already Known.
All that means that sports medicine is something of a slow science: individual providers are using clinical judgement and observing to see what works and drawing on a body of knowledge about what has worked in the past to inform their treatment, but we can’t test or tell you a lot of things.
And that also makes it hard for people who don’t have that professional knowledge to access your own medical information. Because you need basics and context to interpret everything but that information is just in our heads.
Ideally, the point of the professional trainer is just to be efficient: they carry that body of knowledge and fish out what you need when you need it so you don’t have to sit through Human Anatomy & Physiology and SM 101 just to understand what your ankle is doing. In practice, the knowledge often bottlenecks there and it never gets to you.
So you want to search and ask for sources for medical information, but also keep in mind that not all our knowledge is available in a form you’re familiar with, and what is out there might need a lot of context.
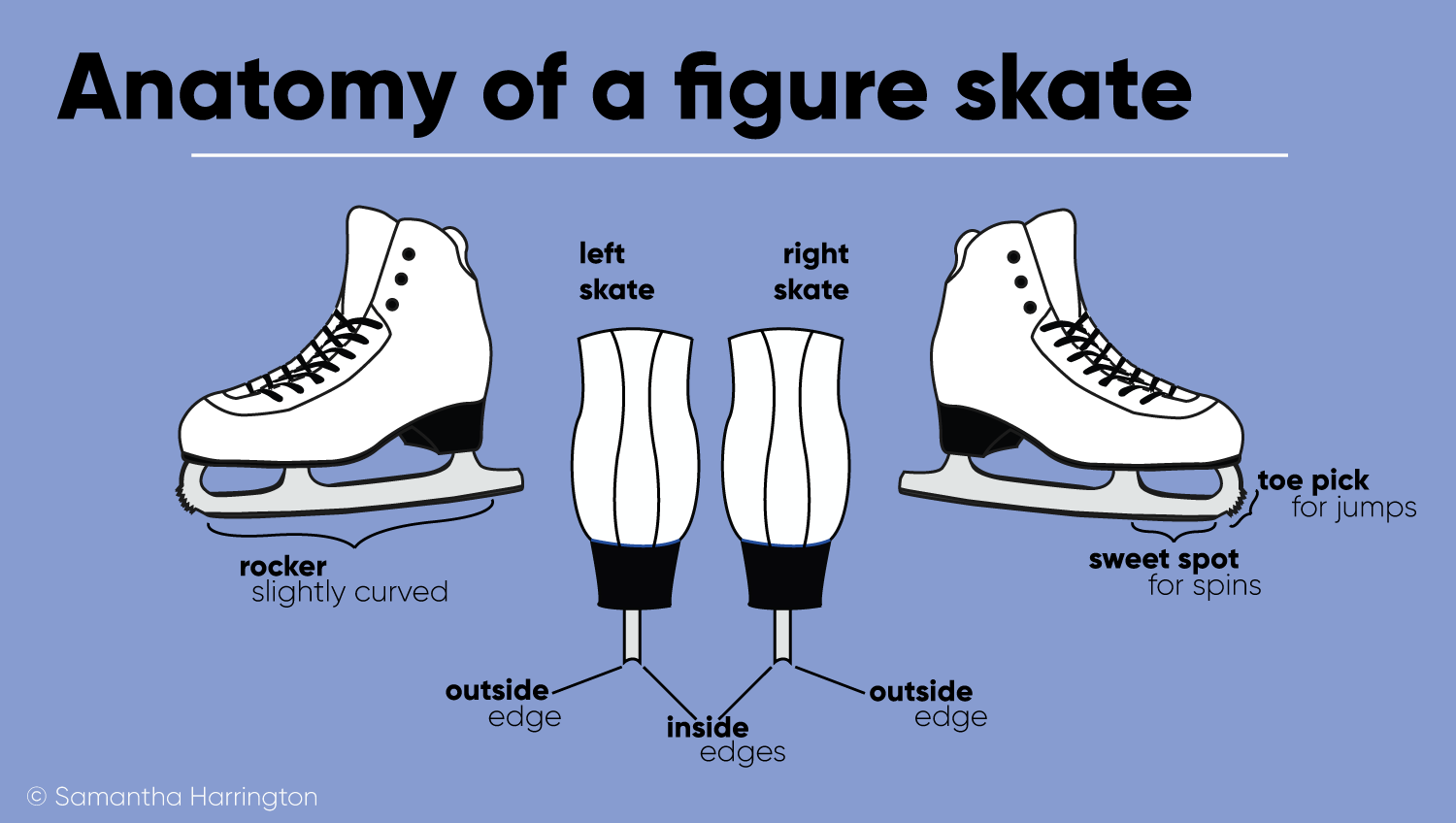
@selasphorus-rufus is spectacular for jumping in to talk about edges: I skimmed over them here and got into it more in a couple replies, because apparently I sure misread the room and thought it would muddy things up.
“if you look at that leg diagram, the tibia is much closer to where the inner edge of the skate is, ergo hockey players would be positioning most of their weight on the tibia as it’s much easier to balance on the inner part of your foot when using the inner part of your foot”
This is a great way to start reading it, and the basic principle is on point.
How To Evaluate Figure Skating Injuries by Rachel Janowicz, DPM gives a quick summary of edgework and how it affects the entire leg; I’m limiting myself to the ankle because the good lord knows I need some limits here, (but you better believe skating-related bone changes work all the way up through your hips and back.)
It’s a little more complex because your ankle is complex. When you use your edges, the sole of your foot doesn’t stay flat and perpendicular to your leg bones: you lift up off the heel and onto the ball of your foot, and your tip the sole of your foot in or out, which is called pronation or supination. That creates an angle between your leg bones and your foot bones.
They’ve drawn a straight line, but his actual feet are slightly, distinctly tipped out as he strides. That supination make an angle with his tibia that makes his medial malleolus (the lumpy end fibula at the inside of your ankle) pop out.
(@angsversteuring and @ismellapples That’s what people are looking at. I also think it looks Completely Normal, but many people have much, much less malleolus, so it looks odd to them.)
The bone there is physically pushed out more. High-top “ankle supporting” skate boots put extra pressure on that prominent point of bone (Both hockey players and figure skaters now wear those, so @ineptshieldmaid and @luckyhorseshoecrab yes, both would see this. There are also other factors for figure skaters but I’m too far gone to get into it call me back and remind me later please). That stress as well as the stress of your strides on the angled bone causes increased bone growth, potentially forming bone spurs or bursae, which all adds to the aesthetic charm of your big honkin skater ankle (Smith, 1990; Luke & Micheli, 1999; Anderson, Weber, Steinbach, & Ballmer, 2004.
Smith, A. D. (1990). Foot and ankle injuries in figure skaters. Phys Sportsmed18(3):73-86.
Luke A. C., Micheli, L.J. (1999). Ankle Swelling – Figure Skating. Med Sci Sports Exercis 31(5):S87.
Anderson, S.E., Weber, M., Steinbach, L.S., Ballmer, F.T. (2004). Shoe rim and shoe buckle pseudotumor of the ankle in elite and professional figure skaters and snowboarders: MR imaging findings. Skeletal Radiology 33(6):325-329
Takebe, K., Nakagawa, A., Minami, H., Kanazawa, H., Hirohata, K. (1984). Role of the fibula in weight-bearing. Clin Orthopaedics Related Res. 184, 289–292
*I suppose we could let the Washington Capitals whack each other, but that would be a kinkier kind of science.
At 23 weeks chances are good that this fetus is being removed because it is:
a) Already dead b) Suffering abnormalities such as it developed no brain, or had a serious genetic condition that would kill it quickly. c) Was actively dying (not dead yet but would be within a few days, 100% guarunteed, 0 chance of saving it) d) Was actively killing the pregnant person.
Late term abortions, as shown here, make up only 1.5% of all abortions. The above four reasons are the only reasons such procedures are performed. Almost every abortion performed after 20 weeks is done on a wanted pregnancy. So you know what that means? You’re calling people who miscarried murderers. You just implied people who had a miscarriage or would have died murderers. How dare you call yourself pro life for that.
Now for the fun fact: They used to use a different procedure for these abortions in which they removed the fetus intact and allowed these people to grieve for the intact fetus, have pictures, etc. Pro lifers decided people losing a wanted pregnancy should not be allowed to grieve an intact fetus and we were left with this.
Congrats. Your movement is the reason they use this one now when people lose a wanted pregnancy late into the pregnancy. Your movement is intentionally making it harder for people to recover from the lose of a much wanted pregnancy. It’s your movement who left grieving people with this instead of allowing them something easier to deal with, something that would let them hold their deceased fetus.
Congrats. If you think you were ‘saving’ something think again. You’re hurting born people. You’re hurting people who lose a wanted pregnancy by shaming this abortion procedure. And you’re movement is the reason this is procedure doctors are forced to use now. You’re probably an awful and mean person to tell people losing a wanted pregnancy that they’re killers.
This is the post that made me pro-choice. Glad to see it still circulating.
I lost a baby brother at something like 14 weeks because he’d attached to the uterine wall backward, and when he started kicking he tore himself away and hemorrhaged to death.
You goddamn “pro-lifers” were ready to let my mother die with him rather than “killing him before God’s time.” He was already dead; it was a matter at that point of him bleeding out. My mother was bleeding with him. My mother was dying with him. And the hospital she was in? That fine pro-life hospital? Refused to let her transfer to another hospital to abort. She had a ten-year-old and an eight-month old at home, but making sure Joey didn’t die “before God’s time” was more goddamn important than making sure my mother survived.
My mother asked the nurse if she’d take pictures, saying that the ultrasound images were really blurry and she’d at least like something to remember him by. The nurse, after Joey was dead and my mom was in recovery, threw pictures on my mother’s bed. This fine pro-life nurse gave my mother pictures of a baby that was jet black where he wasn’t blood red. He didn’t even look human. And she threw the pictures in my mother’s face, like it was her fault that there was a terrible, terrible biological mistake that made it impossible for her baby to survive.
We wanted him. Not that the fact that you’ll notice he already had a name picked out would’ve clued you in. I would have had a baby brother just a year younger than me. My sophomore year in college I spent a lot of time crying alone in the student union, thinking it wasn’t right, it wasn’t fair, I should be taking my brother to dinner with friends or helping him study for his first midterms. I’m a big sister with no little brother to show for it, and there was a year that pain and loss came back eighteen years after the fact to wound me when I least expected it. There was a year when there were songs I couldn’t bring myself to listen to without crying because they reminded me of what I could have had. And I still wish, I still wish, they’d aborted him. Because the end result would have been the same. And my family would have been spared a world of pain believing we were losing brother and mother both. I was in ICU at the time after an allergic reaction that left me unable to breathe. How do you suppose my sister felt? Mother dying, sister dying, brother dead—just a matter of time on that one. Ten years old, watching her entire family struggling to breathe, struggling to live.
And you motherfuckers would call my mom a murderer for this. And you cared more for a baby already dying than you did for the two already born who needed their mom.
Fuck you. You’re not pro-life. You’re anti-woman, anti-family, anti-compassion and anti-love.
Someone on my FB shared this photo and I had to go sit in silence for awhile at the stupidity of her comment that went along with it. Most people don’t wait so late into a pregnancy and randomly decide ‘kill the baby’ because they want to. What the fuck is wrong with people.
Why I will always be pro choice
I’m absolutely crying right now
This really pisses me off, because last year my cousin Emily (Emmie) actually did die from not being able to abort her baby. When she was just under 20 weeks along with her second daughter they found out she had a condition which causes high blood pressure and protein in urine. The doctors gave her like a 5% chance of being able to bring the baby to term with both of them surviving. She and her husband were DEVASTATED.
She regretfully scheduled an appointment to terminate, but people found out. She went to church for comfort, so that she would have people there for her when she would need them but she got the opposite. Her church threatened to ex-communicate her, even though she tried to explain she didn’t want to abort, she had to to survive. People told her that a good mother would be willing to risk her life for her child, and sent her letters saying she was going to hell and threatening to physically attack her if she went through with it. Someone even told her four-year-old daughter, who was really excited about getting a little sister, that “You aren’t going to get a little sister because mommy is going to kill the baby.” They told that to a FOUR-YEAR-OLD! The harassment got so bad that on the day of her appointment, she didn’t go. About a later her liver started to fail, then her kidneys. Within a few days she was dead. They did deliver the baby at 23 and a half weeks, but she didn’t survive more than a few hours.
Of course the church held a big memorial for her and the baby, going on and on about hour strong she was and what a great person and mother she was. And how it was a tragedy that she was taken so young but “god works in mysterious ways.”
BULL FUCKING SHIT! Emmie was already vulnerable and distraught and she went to those people looking for comfort and they turned on her so brutally that she was too terrified and ashamed to have a necessary medical procedure. That’s NOT pro-life. That’s not even anti-choice, because she didn’t have a choice, she NEEDED that abortion to save her life. That is pro-birth. Congrats, the baby was born. She lived for 2 hours and 48 minutes, the entire time in pain, but she was born. Mission accomplished. But now the baby’s dead, Emmie’s dead at only 28 years old, her husband is a widower, and her now 5 year old daughter gets to live the rest of her life without a mother.






{kind=link}